Author: Carlos E Restrepo-Garces MD * 1, Sara Saldarriaga 2, Sergi Boada MD 3
Author Affiliation:
1 Pain Relief Unit, Department of Anesthesia, Clinica Las Americas AUNA, Colombia
2 Medical Student, CES University, Faculty of Medicine, Medellin, Colombia
3 Department of Anesthesiology and Reanimation, Joan XXIII University Hospital, Tarragona, Spain
Competing Interests: The author/s declare no competing interests.
Issue: 04.03
DOI: 10.30756/ahmj.2020.04.03
Received: Sept 24, 2020
Revised: Jan 7, 2021
Accepted: Jan 12, 2021
Published: Jan 25, 2021
Recommended Citation: Restrepo-Garces CE, Saldarriaga S, Boada S. Continuous Sphenopalatine Ganglion Block for Refractory Hemicrania Continua. Ann Head Med. 2020;04:03. DOI: 10.30756/ahmj.2020.04.03
Trigeminal autonomic cephalalgias (TAC) pose a significant challenge for pain physicians. Despite being part of the primary headache disorders, they are uncommon in the general population. Although the literature commonly describes pharmacological management, in refractory patients, interventional pain modalities may be necessary 1.
The most prevalent types of TAC are cluster headaches (CH), paroxysmal hemicrania (PH) and hemicrania continua (HC).
In refractory TAC patients, greater occipital nerve and sphenopalatine ganglion (SPG) block are common interventional pain management procedures 2. In selected cases, SPG neuromodulation may be warranted 3. Unfortunately, such technology is unavailable in many countries.
We would like to present this case of a 31-years-old female with a PH/HC refractory to medical management, including indomethacin 200 mg per day, gabapentin 2400 mg per day and tapentadol 600 mg per day. Interventional pain procedures provided only short-term response to single blocks and radiofrequency ablation of the SPG. After a thorough explanation, a continuous catheter was placed in the Pterygopalatine fossa (PPF) to achieve sustained pain relief. The patient was managed in an inpatient setting for 72 hours.
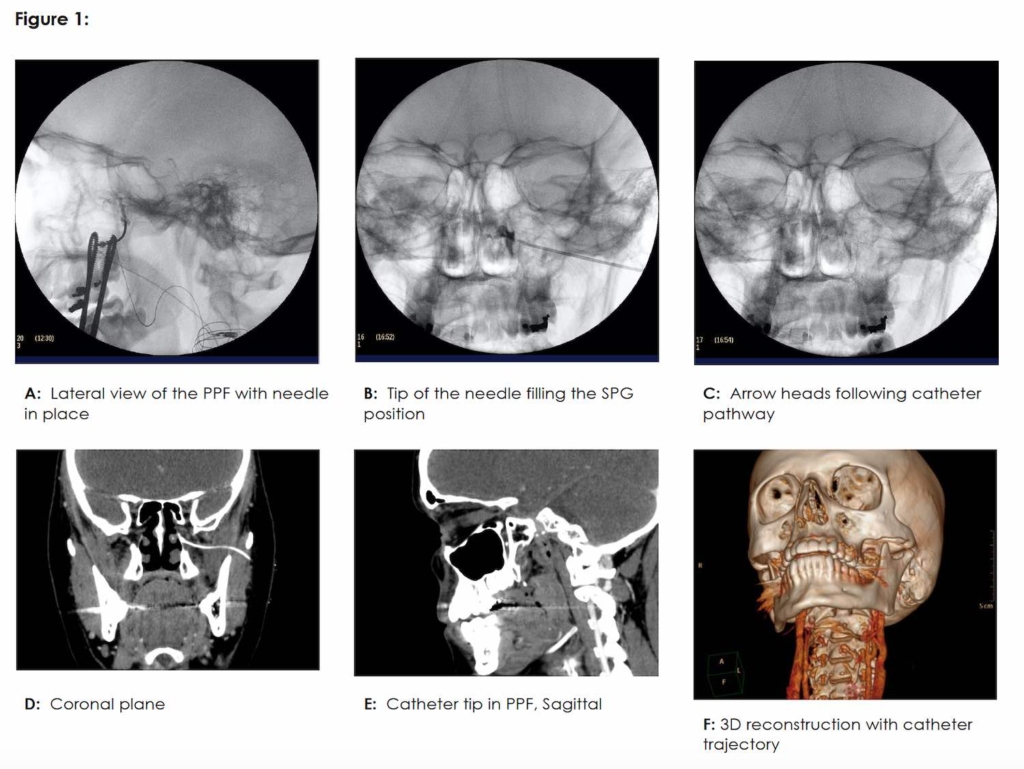
First, the catheter was placed under fluoroscopic guidance using the infrazygomatic approach (Figure 1) with a 18-gauge Tuohy needle and a subsequent Seldinger maneuver to leave a 20-gauge peripheral nerve catheter with catheter tip in the PPF (Contiplex Sonolong Sono, Pajunk, Germany) 4. The final position was confirmed by CT imaging (Figure 1, A-F). A single- injection SPG block was performed using 8 mg of dexamethasone and 3 ml of 0.5% bupivacaine. Then, the catheter was secured using cyanoacrylate (Histoacryl, Braun, Germany) plus a transparent dressing (Tegaderm, 3M, US).
Subsequently, using an elastomeric pump (Baxter Elastomeric Pumps, Baxter, UK) we started a continuous infusion of 0.1% bupivacaine without epinephrine at 0.5 ml/h for the first 24 hours. Then after, we assessed catheter leakage, patient’s tolerance, and analgesic efficacy. Given that the patient reported a pain reduction of less than 50% using the visual analog scale (VAS), the infusion rate was increased to 2 ml/h. The patient reported an improvement of more than 50% in the VAS over the next 48 hours. The infusion was continued at 2 ml/hr for 10 days. No complications were recorded, and the patient remained pain free for six months following the procedure.
To our knowledge, there are no prior reports of this technique. As with other pain conditions, a continuous block will provide a longer-term adjustable response compared with single-shot procedures. However, this technique needs to be validated and currently there are no existing data about the safety of long term SPG infusions. Continuous SPG block could be a feasible intervention in refractory TAC patients.
References
- Gupta R, Fisher K, Pyati S. Chronic Headache: a Review of Interventional Treatment Strategies in Headache Management. Curr Pain Headache Rep. 2019 Jul;23(9):68. PubMed CrossRef
- Narouze SN. Role of Sphenopalatine Ganglion Neuroablation in the Management of Cluster Headache. Curr Pain Headache Rep. 2010 Apr;14(2):160–3. PubMed CrossRef
- Narouze S. Neurostimulation at pterygopalatine fossa for cluster headaches and cerebrovascular disorders. Curr Pain Headache Rep. 2014 Jul;18(7):432. PubMed CrossRef
- Narouze SN. Sphenopalatine Ganglion Block and Radiofrequency Ablation. In: N. Narouze S, editor. Interventional Management of Head and Face Pain: Nerve Blocks and Beyond. New York, NY: Springer; 2014. p. 47–52.
Disclosures
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Declarations
The manuscript has been approved by the ethical research committee and the informed consent has been obtained.
This is an image article and therefore there is no registration in clinical trials.